WHO declares global health emergency over Ebola outbreak in DRC and Uganda
The World Health Organization has declared a public health emergency of international concern after an Ebola outbreak caused by the Bundibugyo virus spread across the Democratic Republic of the Congo and Uganda, with at least 80 suspected deaths reported.
- WHO declares public health emergency of international concern over Bundibugyo virus Ebola outbreak in DRC and Uganda.
- At least 80 suspected deaths and 246 suspected cases reported; officials warn of a potentially larger hidden outbreak.
- No approved vaccine or treatment exists for the Bundibugyo strain, raising containment concerns.

The World Health Organization (WHO) declared a public health emergency of international concern (PHEIC) on 17 May 2026, after an outbreak of Ebola disease caused by the Bundibugyo virus was confirmed across multiple provinces of the Democratic Republic of the Congo (DRC) and the Ugandan capital, Kampala.
The declaration was made by WHO Director-General Tedros Adhanom Ghebreyesus under Article 12 of the International Health Regulations (2005), following consultations with both affected governments and a review of available scientific evidence.
WHO stated the outbreak does not meet the threshold for a pandemic emergency, but warned that available data pointed to a "potentially much larger outbreak than what is currently being detected and reported."
Scale and spread of the outbreak
As of 16 May 2026, eight laboratory-confirmed cases, 246 suspected cases and 80 suspected deaths had been recorded in Ituri Province of the DRC, spanning at least three health zones: Bunia, Rwampara and Mongbwalu.
Two laboratory-confirmed cases were additionally reported in Kampala, Uganda, on 15 and 16 May 2026. Both individuals had recently travelled from the DRC and had no apparent link to one another. One of the two confirmed Ugandan cases has since died.
The Africa Centres for Disease Control and Prevention (Africa CDC) Director-General Jean Kaseya stated that the first cases had emerged in the Mongwalu health zone, described as a high-traffic mining area.
"Cases subsequently migrated to Rwampara and Bunia as patients sought medical care, enabling spread across three health zones," Kaseya said at an online briefing.
A case initially reported on 16 May involving an individual returning from Ituri to Kinshasa was subsequently found to have tested negative for the Bundibugyo virus on confirmatory testing by the Institut National de Recherche Biomédicale (INRB) and is therefore not classified as a confirmed case.
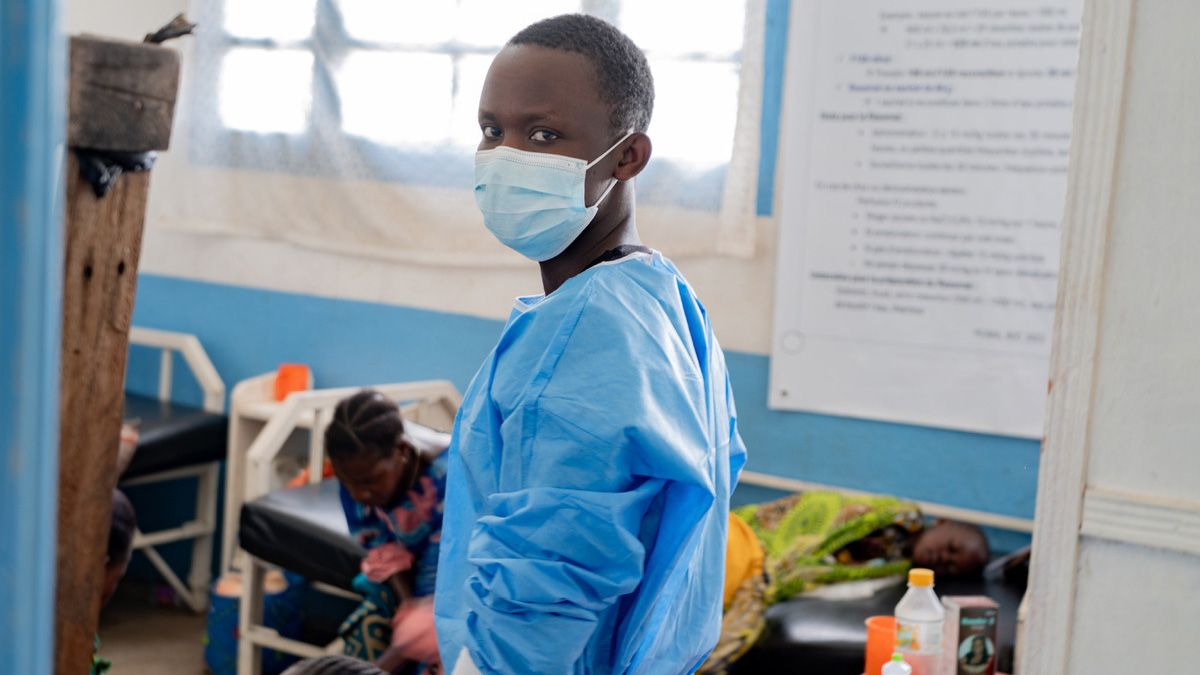
At least four deaths among healthcare workers, in a clinical context suggestive of viral haemorrhagic fever, have also been reported from the affected area, raising concerns over healthcare-associated transmission.
Martyrs' Day postponed as Uganda acts on outbreak risk
In one of the most visible signs of the outbreak's domestic impact, Ugandan President Yoweri Museveni announced the postponement of Martyrs' Day, one of the country's most significant national and religious observances, normally held on 3 June each year at the Namugongo Martyrs' Shrine.
The event typically draws hundreds of thousands of pilgrims from across East Africa, including large numbers travelling annually from eastern DRC — the current epicentre of the Bundibugyo virus outbreak.
In a public address, President Museveni said the decision had been taken following consultations with the national epidemic response task force and religious leaders. He urged pilgrims who had already begun travelling to turn back.
"To safeguard everyone's lives, it is essential that this important event be postponed," President Museveni said, adding that individuals should report any sick persons in their communities and encourage the unwell to seek medical care.
The Bundibugyo strain and why it matters
The Bundibugyo virus is one of three strains of the broader orthoebolavirus family known to cause large outbreaks, alongside the more widely known Ebola virus and Sudan virus. Unlike the Ebola-Zaire strain, for which approved vaccines and treatments exist, there are currently no licensed therapeutics or vaccines specific to Bundibugyo virus disease (BVD).
Amanda Rojek, Associate Professor of Health Emergencies at the Pandemic Sciences Institute, University of Oxford, noted in a statement that "Bundibugyo has fewer proven countermeasures than Zaire ebolavirus, where vaccines have been highly effective in controlling outbreaks."
Prof Raina MacIntyre, an epidemiologist and head of the biosecurity programme at the Kirby Institute, University of New South Wales, said this strain was not the most severe but remained deadly.
"This particular strain of Ebola is not the most severe, but it seems to be killing about 30 per cent of people who have got infected so far," she said, adding that the true case count was "probably more than 300 cases."
Prof MacIntyre suggested the infection had likely been spreading undetected for several weeks prior to detection, noting that reaching a case count of 200 to 300 required sustained community transmission.
Why mortality is high in affected areas
Paul Griffin, an infectious diseases expert at the University of Queensland, attributed the high mortality rates in part to the severely resource-constrained environment in which cases are occurring.
"We do have to remember that those quoted mortality rates are in people that are infected in very resource-poor settings, so often don't even have access to simple things like intravenous fluids, which can make a big difference," he said.
Ongoing insecurity in Ituri Province, where militant activity continues to restrict surveillance and rapid response operations, further complicates containment efforts.
WHO also identified high population mobility, the urban and semi-urban character of current hotspots, and a large network of informal healthcare facilities as compounding risk factors, drawing comparisons with the large Ebola epidemic in North Kivu and Ituri in 2018 and 2019.
How Ebola spreads
Ebola viruses spread through direct contact with bodily fluids from an infected or deceased person. Transmission can also occur through sexual contact, contaminated needles, or contact with infected animals such as fruit bats, primates or apes.
Prof MacIntyre noted that funeral practices in many affected communities, which may involve handling or bathing the deceased, had historically contributed to transmission. Healthcare workers are also considered at elevated risk, particularly when a diagnosis has not yet been established and full personal protective equipment (PPE) is not being used.
What WHO's declaration means
The PHEIC declaration represents the WHO's highest level of alert short of a pandemic emergency. It signals that an event is serious, carries a risk of international spread and requires a coordinated international response.
"Part of the reason, once again, of declaring the public health emergency of international concern is to make sure there are better resources available where these cases are to try to improve some of those outcomes," Prof Griffin said.
WHO advised that no country should close its borders or restrict travel and trade, describing such measures as scientifically unfounded and counterproductive. The agency noted that border restrictions tend to divert population movement to informal, unmonitored crossings, thereby increasing the risk of further spread.
Countries sharing land borders with the DRC have been advised to urgently enhance preparedness, including active surveillance, laboratory access and the establishment of rapid response teams.
WHO's Director-General will convene an emergency committee as soon as possible to advise on temporary recommendations for all States Parties in responding to the outbreak.
Situation in brief
The outbreak represents only the third recorded instance of Bundibugyo virus disease since the strain was first identified. The high positivity rate of initial samples — eight positive results from 13 collected across various areas — alongside the confirmation of cases in both Kampala and Kinshasa suggests the true scale of the outbreak may substantially exceed current reported figures. WHO indicated it would update its guidance following the emergency committee's deliberations.